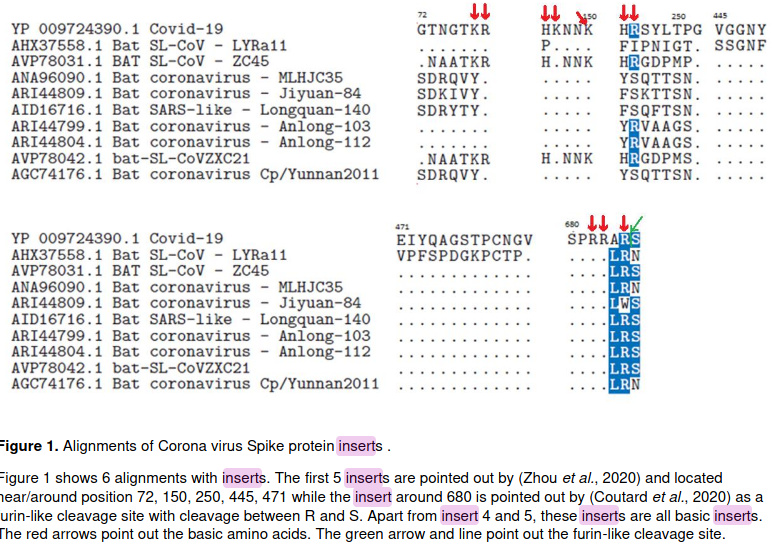
So the proteolytic furin cleavage site is exactly what those virologists were talking about when they said someone inserted a part of HIV virus into SARS-COV-2.
Looks like a coronavieua vaccine is what we need.
Methods: Monocentric retrospective study conducted from 2th March to 17th April 2020, in adults hospitalized in a tertiary hospital for COVID-19. Patients characteristics were compared between groups depending on the therapy received (HCQ/azithromycin taken ≥ 48 hours or other treatment).
Outcomes were evaluated from admission, by the need for intensive care unit (ICU) support and/or death. Univariate analyses were performed using non-parametric tests and confirmed by a multiple logistic regression using Pearson correlation test.
Results: Among 132 patients admitted for COVID-19 in the medicine ward, 45 received HCQ/azithromycin ≥ 48 hours, with a favorable outcome in 91.1% of cases (OR=6.2, p=0.002) versus others regimen (n=87).
Groups were comparable at the baseline in terms of age, sex, comorbidities, extend in thoracic imaging, and severity. Among patients that required to be transferred to ICU (n=27) (for mechanical ventilation), median delay for transfer was 2 days (IQR 1-3).
We report only 1 patient that presented an adverse event (a prolonged QT interval on EKG) that required to discontinue HCQ.
Conclusion: The present study suggests a potential interest of the combination therapy using HCQ/azithromycin for the treatment of COVID-19 in in-hospital patients.
We shouldn’t politicize medicine. The author of this study received so much flame that he had since chosen to undisclose his paper until its been peer-reviewed, which is very unusual for COVID-19 related research, since time is of the essence here.
We should let valid studies and numbers do the talking.
A vaccine study by Norwegian virologist Birger Sørensen, where he also pointed out that certain sections of SARS-COV-2 is likely human inserted.
Sørensen said, “When we technically describe the virus, we see that it has not come about in a natural development. It’s done by Americans and Chinese, as part of what’s called “gain of function” studies. It is done all over the world. You say you don’t, but it happens all the time in advanced labs.”
…
The authors also highlight the lack of mutation since its discovery, which suggests it was already fully adapted to humans.
These data reveal the biological structure of SARS-CoV-2 Spike and confirm that accumulated charge from inserts and salt bridges are in surface positions capable of binding with cell membrane components other than the ACE2 receptor. We have also looked at the naked coronavirus spike protein as a concept for the basis of a vaccine, which we have rejected because of high risk of contamination with human-like epitopes. Analysis of the Spike protein of SARS-CoV-2 shows 78.4% similarity with human-like (HL) epitopes. For the avoidance of confusion, a standard protein blast searches for functionalities and homologies to other proteins.
However, antibodies can only recognize 5-6 amino acids and therefore a 6 amino acid rolling window search for antibody epitopes was performed. A search so tailored to match against all human known proteins will give a 78.4% human similarity to the SARS-CoV-2 Spike protein, i.e if all epitopes on the 1255 amino acid long SARS-CoV-2 Spike protein can be used by antibodies then there will be 983 antibody binding sites which also could bind to epitopes on human proteins. This is what we did and found.
Well, we know that it’s already mutated.
https://www.post-gazette.com/news/science/2020/05/05/coronavirus-strain-study-scientists-new-mutant-more-contagious/stories/202005050156
Covid - 19 and blood type.
https://www.bloomberg.com/news/articles/2020-06-08/23andme-provides-more-evidence-that-blood-type-plays-role-in-virus
WTF, isn’t baldness punishment enough?
I first saw this from a hair transplant clinic ![]() I’m not sure if getting a hair transplant helps, as hair loss if probably only the symptom. It’s could be related to DHT in the body if balding is correlated to severe symptoms.
I’m not sure if getting a hair transplant helps, as hair loss if probably only the symptom. It’s could be related to DHT in the body if balding is correlated to severe symptoms.
Apparently your infected cells would grow testicles to reach for other cells to infect.
It’s more and more clear that antibody that we get from infection or vaccines aren’t going to be long lasting, as is the case with other similar coronaviruses.
It binds too well to humans right off the gate to not be engineered this way.
I feel like people want this to fail because it’s so cheap and widely available. We already found data was faked. Now more studies show it works.
https://www.ijidonline.com/article/S1201-9712(20)30534-8/fulltext
I’ve been wondering if something like this could apply to Taiwan on a large scale.
People who sneezed in crowded buses, kids who went to school despite symptoms of cold, etc. may have helped us.
Edit: Wouldn’t that be something if Taiwan came up with the most effective vaccine and did so in a timely manner (for example, by the end of the year).
People who went to work or class sick, spreading the joy, yeah, build up the immunity bank. 
I think the issue with that theory is that you’d need to demonstrate that there’s something relatively unique about Taiwan in terms of the T cell distribution in the population, i.e., a significantly higher proportion of people having some degree of preexisting cross-reactive T cell immunity to SARS-CoV-2.
I’m not sure how that would have come about. For example, is there any evidence that common colds are more…err, common in Taiwan than the US, Europe, China, or anywhere else? (I feel like I get colds less frequently here than anywhere else I’ve lived, personally; n=1.) I also think that people with colds tend to be more responsible here than in other places (wearing masks when sick, etc.). For most of my life in the UK, I don’t think it would ever have occurred to me to stay home from school/uni/work because I had a cold and wanted to protect others, and I think that’s a pretty common attitude - occasional colds are just part of life.
Or that the typical strains prevalent in Taiwan include a relatively high proportion of coronaviruses (cf. rhinoviruses, adenoviruses, influenza viruses, etc.) that might grant partial cross-immunity? I assume that the prevalent strains in a particular year vary with geography and human genetics, but given the degree of human movement/travel over the last few decades I’d be surprised if there’s a massive difference in strain distributions between Taiwan and, say, China or HK or the Philippines.
That’s what I was thinking, or perhaps a particular recent strain. Just a thought, indeed one would have to demonstrate it ![]() We do seem to have an uncanny ability to ward off community transmission.
We do seem to have an uncanny ability to ward off community transmission.